“From the view of psychological factors in suicide, the key element in every case is psychological pain; psychache. All affective states (such as rage, hostility, depression, shame, guilt, affectiveness, hopelessness, etc.) are relevant to suicide only as they relate to unbearable psychological pain. If, for example, feeling guilty or depressed or having a bad conscience or an overwhelming unconscious rage makes one suicidal, it does so because it is painful. No psychache, no suicide”. Edwin Shneidman, Suicide as Psychache p56
Psychache is the unbearable guilt, despair, hopelessness, shame, pain, depression, and press one feels when thinking about suicide. It is the corner stone of what this paper is about. The pain of the mind can cause constriction, a narrowing of view of things. It can also lead to perturbation (an unrest that causes one to feel like doing something to alleviate the uneasiness one feels) and also to press, which is also known as stress or the pressure and weight one feels under. The combination of these three things, press, perturbation, and psychache is what is known as the cubic model of suicide.
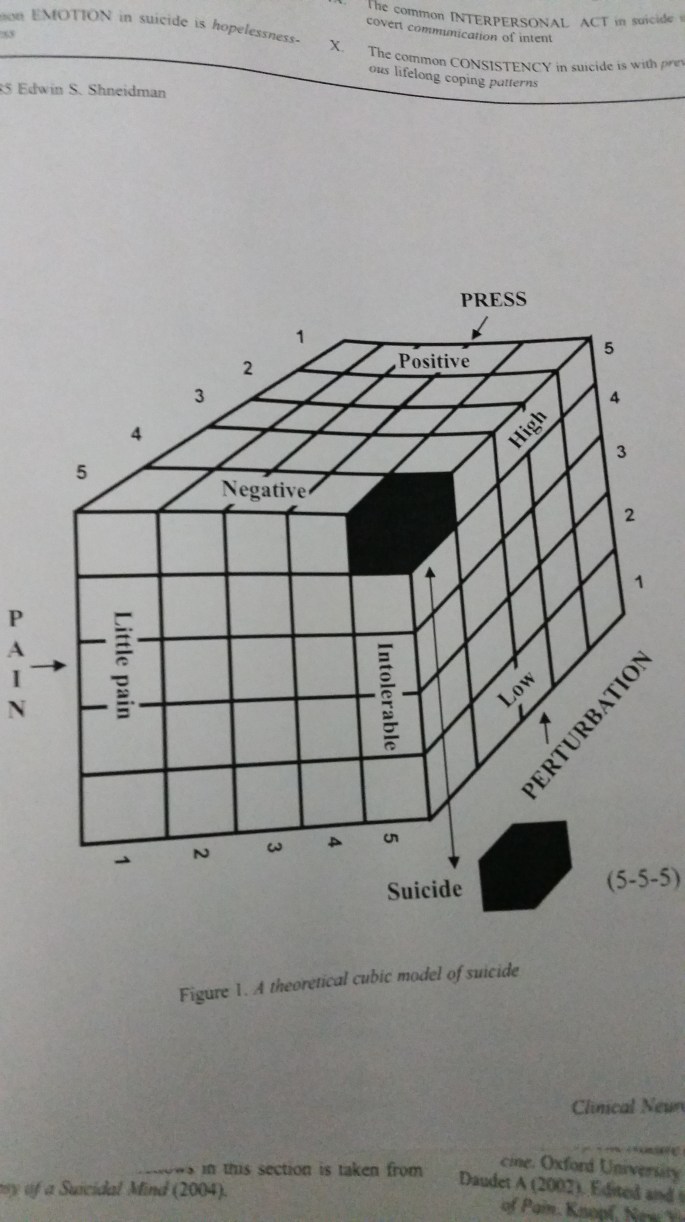
The cubic model of suicide is a 1-5 rating of the three things I just mentioned. The higher the rating, the higher the likelihood of suicide. The worst rating is a 5-5-5 scenario and suicide will be imminent. It is important to rate these items when dealing with a suicidal person. It will validate what they are feeling and make them feel at ease in talking about what is causing them to feel so pressured and hurt to make them think of killing themselves.
When dealing with constriction, the dichotomous thinking that a) suicide is the only way out or b) things are always going to stay the same, it is important to always bring in more options to the person so they can see things differently. In his book Suicide as Psychache, Shneidman gives the example of a young pregnant woman who was thinking of killing herself with a handgun. She couldn’t have the baby so therefore in her mind, suicide was the only way out. After discussing several options with her (calling her parents, having the baby and giving it up for adoption, discussing the situation with the baby’s father, etc.), it was agreed that the woman would call the baby’s father. Suicide was no longer the number one item on the list. To prevent a mishap, Shneidman did take the gun away from the woman. An excellent example about means restriction.
In almost every suicidal thinking, there is some measure of lethality and perturbation. You can have high lethality and high perturbation, but you don’t always have high perturbation with high lethality. Perturbation, as described above, is very much like anxiety. It is a perturbed feeling that causes one to feel pressured to do something. Lethality is the doing something.
Also in every case of suicidal thinking is the frustrated needs that bring about the suicidal feelings.
ABATEMENT The need to submit passively; to belittle oneself
ACHIEVEMENT To accomplish something difficult; to overcome
AFFILIATION To adhere to a friend or group; to affiliate
AGGRESSION To overcome opposition forcefully; fight, attack
AUTONOMY To be independent and free; to shake off restraint
COUNTERACTION To make up for loss by retrieving; get even
DEFENDANCE To vindicate the self against criticism or blame
DEFERENCE To admire and support, praise emulate a superior
DOMINANCE To control, influence, and direct others; dominate
EXHIBITION To excite, fascinate, amuse, entertain others
HARMAVOIDANCE To avoid pain, injury, illness, and death
INVIOLACY To protect the self and one’s psychological space
NURTURANCE To feed, help console, protect, nurture another
ORDER To achieve organization and order among things and ideas
PLAY To act for fun; to seek pleasure for its own sake
REJECTION To exclude, banish, jilt, or expel another person
SENTIENCE To seek sensuous, creature-comfort experience
SHAME-AVOIDANCE To avoid humiliation and embarrassment
SUCCORANCE To have one’s needs gratified; to be loved
UNDERSTANDING To know answers; to know the hows and whys
These twenty needs are what Shneidman has called the essential ones when people are suicidal. Most of them are not all twenty but five or six as it pertains to the individual. “The prevention of suicide with a highly lethal person is then primarily a matter of addressing and partially alleviating those frustrated psychological needs that are driving that person to suicide. The rule is simple. Mollify the psychache”. (p53) Shneidman believed that these frustrated needs are what caused psychache.
I believe there should be another need, validation. Everyone needs to be validated in order to feel secure and feel okay. Without this, most people feel shamed and dumb, that what they are feeling or experiencing has no meaning or purpose. They may also feel empty and alone as no one understands what they are going through. This need when frustrated or thwarted can lead to suicide.
Shneidman, Edwin. Suicide as Psychache. 1993. Jason Aronson, Inc.

You must be logged in to post a comment.