My thoughts about Zero Suicide as a person with Lived Experience
There has been a lot of talk on Twitter about Zero Suicide and it’s mission to reduce the suicide rate to zero, because 1 is just too many. At first, I was appalled that clinicians think that is possible. I for one think that it is outrageous because there is always going to be someone who dies by suicide. Maybe not in their organization but outside their organization. But then I learned that it’s not an individual’s practice but an organization or health system that strives to achieve this goal. They have trainings and meeting with those in the suicidology world.
Something kept bugging me about this. I kept quiet because I didn’t want to anger those that are for it, though I think there are a few blogs that I wrote about it before I understood the mission. While talking to a friend that is a suicide loss survivor, the bells went off. She said that it goes against Shneidman’s questions, where do you hurt and how can I help?
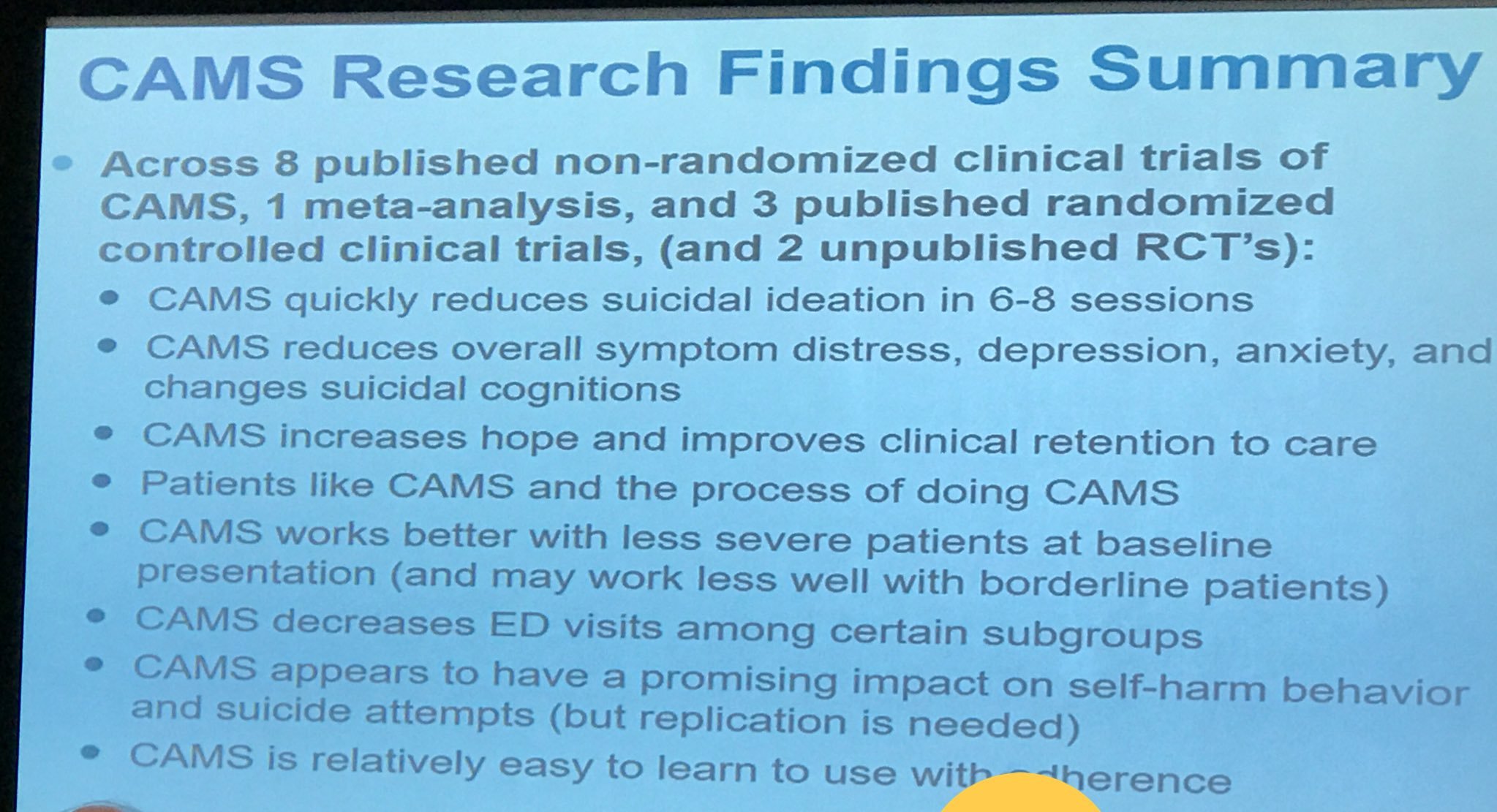
I am a big supporter of Dr. David Jobes work with his framework called CAMS (Collaborating, Assessment, and Management of Suicidality). I don’t know if Dr. Jobes trains these Zero Suicide clinicians. And even if they are trained, I am not sure it will be used. Most clinicians have the attitude that their skills on suicide risk are good enough when it could be faulty. Worse, they go through the training yet don’t use what they are taught. That drives me up the wall. Why bother going to a training (unless it’s a mandatory thing) if you aren’t going to take away from it?
I really think CAMS is a tried and true framework to prevent suicide based on my experience of using it in my former therapy. I also used the Suicide Status Form. Unfortunately, my therapist did not want training in CAMS and we drifted apart, thus ending our relationship. We did, while we worked together, use the initial and tracking forms but unfortunately, we never got to the outcome form. She wasn’t committed enough to see it through and that kind of pissed me off. Every time I had a suicidal episode, she just wanted to know one question on the form, The one thing that would help me no longer feel suicidal. It is an open ended statement where the client fills in their thoughts on the matter. Unfortunately, I could never come up with a satisfactory answer as I really didn’t know the reason for my suicidality. I just wanted to die and that was that. I wrote a blog about CAMS if you would like more information about how it is formed and the use of the Suicide Status Form.
I went on the website for Zero Suicide but could not seem to find the specific training that they went through. From what I gathered on Twitter from their live tweets, some of it is CAMS and some of it is using risk factors for suicide. Unfortunately, risk factors alone are not predictive of a suicide attempt. CBT has been useful in reducing suicide attempts but not all clinicians are trained in this modality. The book by Craig Bryan on CBT for preventing suicide attempts is a good book to learn more about it. I also wrote a review on the book that you can see here.
The other thing that gets me is that no where among Zero Suicide is there talk of a person’s psychological pain. There are measures, if you look for it. Dr. Holden at Queen University in Canada has created a scale to measure what Dr. Shneidman calls psychache. See my review on the research article for more information. I think it is a good psychometric to gauge a person’s level of suicidality and pain, which ultimately leads to thoughts of suicide. This must be included in any talk of preventing or intervention of suicide and also postvention, should a suicide attempt occur.
My final thoughts of Zero Suicide is that it is a novel idea but as Dr. Shneidman says, “How many suicides do you want, and I say I don’t want any, but I want there to be the freedom to do it. I study suicide but I am not pro-suicide. I’m for suicide prevention.” I share his sentiments. I do not like the talk of “suicide is not an option”. To me, that is hindering free will. I do hope the rate of suicides goes down, but the way that health care and mental health are going, I think there will be more before it lowers, especially among the chronic pain patient population.

You must be logged in to post a comment.