I had an appt with a nurse practitioner that apparently got her license from a cracker jack box or maybe the Boston Globe. She was insistent on me having plantar fasciitis even though my PT ruled it out but didn’t I read the newspaper, not a medical journal, saying that plantar fasciitis is the new back pain?? Are you fricken serious? I didn’t know reporters had their medical degree. Also pissed me off that she thought unilaterally and bilaterally were the same. Ugh!!!!! I had to literally fight for an MRI. She wanted an xray and didn’t even ordered that right as they xrays the outer part of my ankle not the inner where the damn lump is!!! I am so frustrated. I got to call radiology to see if I can have the MRI sooner than next week and during daylight hours. I might go to a different site. Ugh!! Oh and she was telling me the same damn things to do my PT has been telling me. Guess she was deaf on that part.
Oh and the kicker was that she walked in asking if I was having surgery. When I said no, she said you aren’t having gender reassignment surgery? And then she got all concerned and crap like she never had a transgender patient before. Omg I am not a specimen for your study!!! I got very upset by this behavior. I mean, shit. Seriously? I emailed my psychiatrist to ask her what to do. I want to file a report on her as I think what she did was inappropriate. I mean, hell, I was seeing her for foot pain, not a transgender issue! I am so pissed. I hate that she was so dismissive about what I was telling her about being in physical therapy and then dismissing what my PT said about me not having plantar fasciitis. She just wasn’t hearing me and I am glad she ordered the MRI. I already got a report on the X-Ray and surprise, nothing was revealed except for some spurs that have been there for a while.
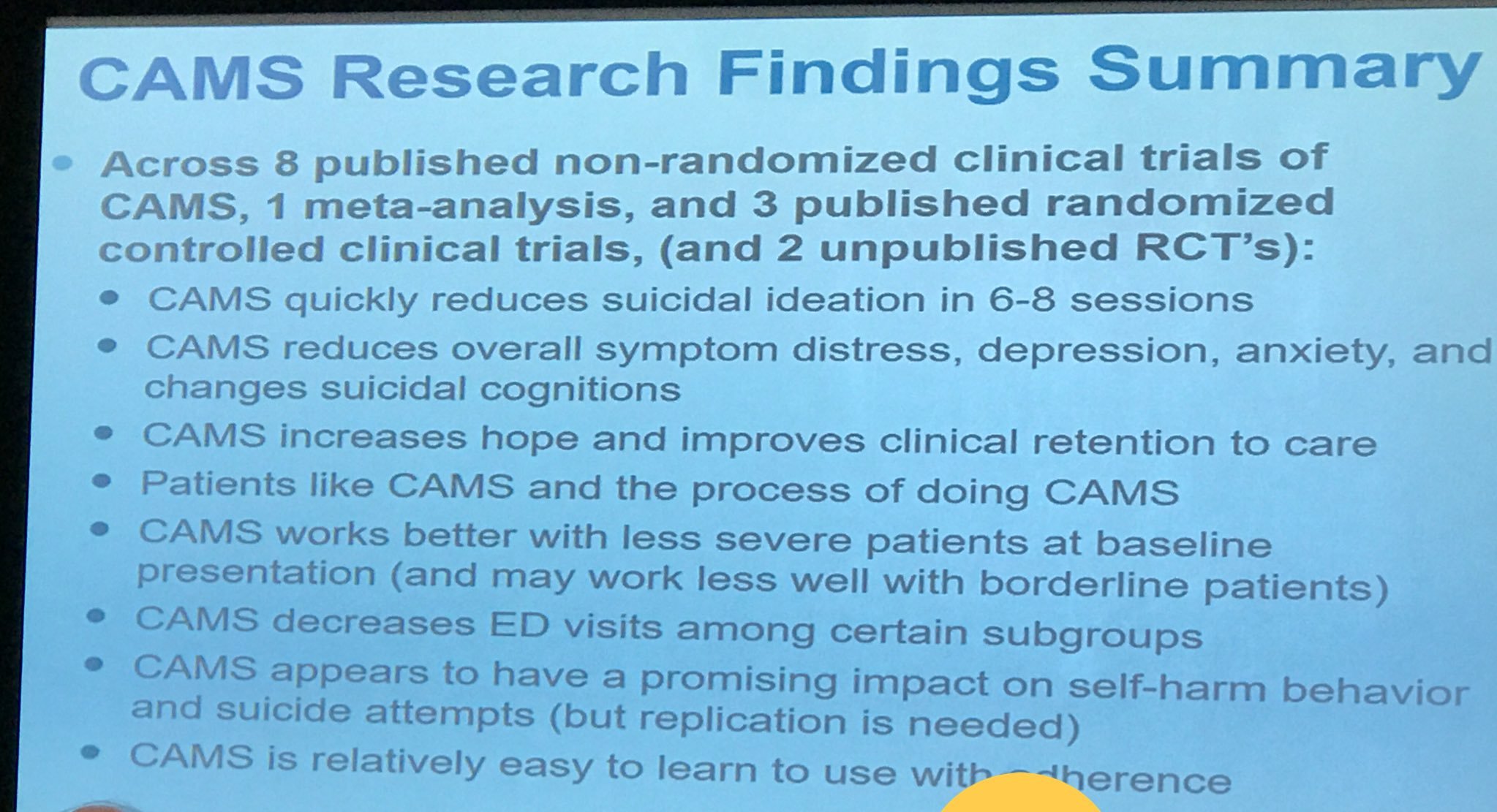
I had a webinar when I came home on CAMS, the Collaborative Assessment and Management of Suicidality. OMG It was like having Dr. David Jobes in my room! It was awesome. I love him so much and have so much respect for him. He basically covered all that I know about CAMS. I love the new research he is doing. Sadly, one of the trials had two suicides. It is a risk but sadly not something you want to see. I wish I could share this with my current therapist but he is so anti-CAMS it isn’t funny. He just thinks talking about things is the answer. I know it is my fault in keeping him but fuck, there aren’t a lot of therapists taking new clients AND wanting to deal with chronic suicidality! I had one therapist not call me back in the Harvard area. I tried out of my comfort zone and that hit me in the ass with a don’t come back. I wish someone was dealing with suicidality in clients rather than just passing them off. If I could sprinkle some of Jobes’s kindness and humanity I would. It isn’t something I take lightly. I have been in the model of what he teaches and want to spread it around but hell, some therapists like the one I was seeing before my current one, was adamant about learning something new. In her words, she wasn’t a suicidologist so she didn’t have to learn it so what that said to me was if she had another client that was suicidal, she was NOT using CAMS/SSF with them. It makes me sad that there is this level of what you think a therapist should be and the reality is they just don’t exist. I don’t know why people become therapists if they aren’t willing to deal with the hard issue of suicide. I don’t know, maybe I have it backwards.
I saw a sign at my PCP’s office that they are moving location, and it is not even within their building. It is a building like 4 blocks over from the train station. I can’t walk there. Maybe on a good day, but those days have been so rare lately that I seriously doubt if I am sick, I will be able to make it. I think there is another way of going there. I just have to find out if the shuttle from another train station still goes by there, and where that stop is as the last time I was in that area, there was construction which had the sidewalk blocked off. This sucks because it adds to my commute and worse, no Starbucks, LOL
I just wrote a thread on Twitter and I am going to paste it here. I think it is important:
“I’ve been thinking about the @UniteSurvivors webinar with @lab_jobes and what he was saying about drivers (what drives ppl to suicide) and how those with lived experience can help. It took me to all the times the past 2 years I’ve been in horrible suicidal depressions/states, mostly due to my chronic pain. Dr. Jobes talked about a “life worth living”. Frankly I don’t even have a day worth living but somehow I am still here. I don’t want to be. I am in a chronic pain flare right now. My thoughts instantly go to suicide because it feels like my bones are being crushed and I am being stabbed in my ankle. How do you survive this while being suicidal? Frankly I don’t have a clue. It is probably because I don’t have lethal means near me when I flare (whether consciously or subconsciously I am not sure). I don’t have a large dose of meds by my bedside or knives. I don’t own a gun, though I sometimes wish I did. Guess these small measures have kept me here. My blog where I can write to Express myself. Have online connections to my support group which is invaluable. Different time zones are a life saver. B/c when it is 3 am, no one is up Boston time. I’ve learned to do this not through a therapist or hospitalization but mostly on my own. And having my psychiatrist email at 2 am is handy. Thank you Dr. Dave for CAMS and the SSF. It combines my thoughts of suicides to practical practice. I know I wouldn’t be here without it. I should add I am an autodidact suicidologist.”
I just read what I wrote and though some of it doesn’t make sense, I didn’t want to fix it because the essence of what I am saying is there. Anyways, that is all I have for today. There is a huge thunderstorm happening right now and I want to publish this before I lose power, if that should happen. Go SOX!!!!!

You must be logged in to post a comment.